Siderosis bulbi is a chronic pigmentary degenerative process following the retention of an iron-containing foreign body. It can lead to sight-threatening complications.

what is Siderosis Bulbi?

Siderosis bulbi is a rare but significant ocular condition characterized by the deposition of iron in the various structures of the eye. It typically results from a retained, iron-containing intraocular foreign body (IOFB) or from repeated exposure of the eye to iron particles. Over time, iron accumulates in ocular tissues, leading to a range of clinical manifestations that can compromise vision.
Pathophysiology
- Introduction of iron into the eye
The most common cause of siderosis bulbi is penetrating ocular trauma involving an iron-containing foreign body (e.g., a small splinter of steel). Once inside the eye, the metal gradually corrodes, releasing iron ions (Fe²⁺ and Fe³⁺) into the intraocular environment. - Deposition in ocular tissues
- Iris: Iron deposition can lead to heterochromia (difference in iris color) and can affect pupillary reactions.
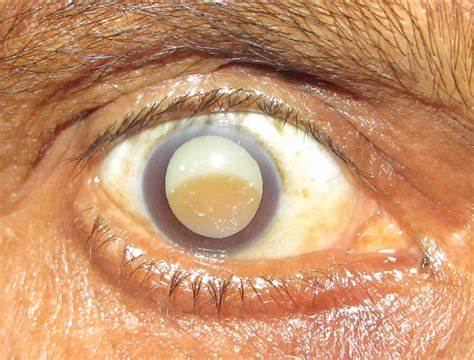
- Lens: Iron can deposit in the lens epithelium, causing the formation of characteristic reddish-brown or “rust” opacities, potentially progressing to cataract formation.
- Retina and Retinal Pigment Epithelium (RPE): Iron preferentially accumulates in the RPE and neural retina, which can disrupt normal photoreceptor function and gradually lead to visual decline.
- Other structures: The cornea, trabecular meshwork, and vitreous can also be affected, although the changes are often more subtle.
- Toxicity
Iron in excess generates free radicals that cause oxidative stress, damaging cellular membranes and organelles. This oxidative damage contributes to cell death in the retina and other structures, ultimately impairing visual function.
Clinical Features
- Early signs
- Iris discoloration (often a rusty or brownish hue)
- Mild visual disturbances
- Subtle lens opacities
- Progressive changes
- Cataract: Opacification of the lens can progress, resulting in reduced visual acuity.
- Retinal changes: Electroretinogram (ERG) abnormalities are often one of the earliest indicators of retinal involvement, even before overt fundoscopic findings are visible.
- Glaucoma: Iron deposition in the trabecular meshwork may lead to increased intraocular pressure.
- Advanced disease
- Significant vision loss due to retinal degeneration and/or dense cataract.
- Severe ocular involvement that may culminate in optic atrophy if not diagnosed and managed promptly.
{kind=link}
Diagnosis
- Clinical History and Examination
- History of ocular trauma involving metal fragments is a key clue.
- Slit-lamp examination can reveal iris color changes, lens opacities, or corneal deposits.
- Fundus examination may demonstrate pigmentary changes in the retina.
- Imaging Studies
- X-ray Orbit: Can help identify the presence of a metallic intraocular foreign body.
- CT Scan: More sensitive than X-ray for detecting metal fragments and assessing their exact location.
- Ultrasound B-scan: Useful in cases where the ocular media are not clear (e.g., dense cataract or vitreous hemorrhage).
- MRI: Generally avoided if a metallic IOFB is present because of the risk of movement or heating of the fragment; however, when used cautiously in specific cases, advanced MRI sequences may help characterize the metal composition.
- Electroretinography (ERG)
- ERG is crucial for detecting early retinal changes. A reduction in ERG amplitude can be the first sign of siderosis bulbi, prompting further investigation even in the absence of significant clinical findings.
Management
- Removal of the foreign body
- The cornerstone of treatment is the prompt surgical removal of the iron-containing IOFB. Delayed removal increases the risk of iron-related tissue damage.
- Approaches include pars plana vitrectomy for posterior segment foreign bodies or other surgical techniques depending on the location.
- Supportive therapy
- Topical and systemic steroids may be used to reduce inflammation.
- Monitoring of intraocular pressure (IOP) is essential, as iron deposition can precipitate secondary glaucoma.
- Prognosis
- Early detection and removal of the iron foreign body greatly improve visual outcomes.
- Once widespread retinal toxicity has occurred, visual recovery can be limited even after removal of the offending IOFB.
Conclusion
Siderosis bulbi is a serious, vision-threatening condition resulting from iron deposition in ocular tissues, typically following penetrating injury involving iron-containing foreign bodies. Early recognition, aided by clinical examination and key diagnostic tests such as ERG, can prevent irreversible tissue damage. Prompt surgical intervention to remove the offending fragment remains the gold standard of treatment.
References
- Bowling, B. (2016). Kanski’s Clinical Ophthalmology: A Systematic Approach (8th ed.). Elsevier.
- Khurana, A. K. (2019). Comprehensive Ophthalmology (6th ed.). Jaypee Brothers Medical Publishers.
- Agarwal, S. & Agarwal, A. (Eds.). (2011). Manual of Ocular Diagnosis and Therapy (6th ed.). Lippincott Williams & Wilkins.
- American Academy of Ophthalmology (AAO). (2023). Basic and Clinical Science Course (BCSC) Section 10: Glaucoma. AAO Publications.
- Duke-Elder, S. (1967). System of Ophthalmology, Vol. XIV: Injuries. Henry Kimpton Publishers.
Discover more from An Eye Care Blog
Subscribe to get the latest posts sent to your email.
You must be logged in to post a comment.